Name
Lab
Section
![]()
Range of Motion/Flexibility
Purpose: To develop a greater
understanding of the nature of flexibility and how it is measured.
Dress: Shorts, t-shirt
Equipment: Goniometer, lab handout, textbook.
Objectives: At
the completion of this laboratory, you should be able to:
1.
Define the
following terms:
range of motion (ROM) active stretching
flexibility passive stretching
active ROM static stretching
passive ROM dynamic (ballistic)
stretching
active insufficiency proprioceptive neuromuscular facilitation (PNF)
passive insufficiency static ROM
dynamic ROM
2.
Determine active
and passive ROM by means of orthopedic goniometry.
3.
Identify an
average ROM of the shoulder, elbow, hip, knee, and ankle in the sagittal plane.
4.
Identify several
methods for assessing joint
5.
Identify which
stretching technique is most effective in increasing
Background
Information:
Range of
motion (ROM) is a description of how much movement exists at a joint. Rotation
is the typical movement at a joint. This is called “angular” movement. Because
the movement is angular, the unit “degree” is used when measuring ROM rather
than inches or millimeters. ROM can be measured as either active or passive.
Active ROM is created by the person contracting the muscles around that joint.
Passive ROM is created by an external force pushing on the body around the
joint (e.g., a partner, an opponent, a piece of equipment). Passive ROM is
always greater than active
Joint ROM
can be assessed through a variety of methods. In PEP 201, you performed several
field tests that are used to measure flexibility at different joints. The
advantage of these field tests is that they can be easily administered to large
groups of people with little equipment and training. However, as you learned in
PEP 201, there are also limitations to these tests. To overcome these
limitations, clinicians and researchers have developed a number of somewhat more
sophisticated devices to measure ROM which provide
greater accuracy with little increase in the complexity of the equipment and
training required. These devices include goniometers
(electro-, protractor, pendulum), inclinometers, and
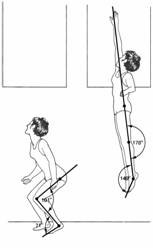
hygrometers. The most accurate techniques for measuring ROM (particularly
dynamic ROM) include measurements of joint angles from arthrographs,
radiographic images, photographs, and video (see figure to the left). However,
these techniques require expensive, complex equipment and extensive training.
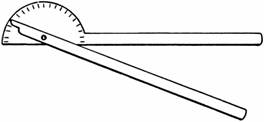
In this lab, you will learn to measure ROM using a protractor goniometer, which is simply a protractor designed for use
on the human body (see figure below to the right).
 There are 3 typical methods used today for
flexibility training: static, dynamic (ballistic), and proprioceptive
neuromuscular facilitation (PNF) stretching. Because temperature affects the
extensibility of the soft tissues around the joint, completing 5 minutes of
warm-up (light aerobic exercise) is recommended before performing flexibility
exercises. Static and dynamic stretching are both effective means of increasing
flexibility, but generally static stretching is considered safer and results in
less soreness of muscles. Dynamic stretching recruits the muscle spindle to
reflexively cause contraction just after the fast stretch. This may result in
small muscle tears in the muscle due to a fast/forceful transition that may not
be timed perfectly. The slow or static stretch also recruits the muscle
spindle, but at a lower response intensity so that tearing is minimized or
eliminated. Holding a stretched position for 10-30 s is usually effective. PNF
may be the most effective method that results in the least amount of
post-stretching soreness. There are several methods of engaging in PNF. Two of
these include contract-relax (CR) and contract-relax antagonist contract
(CRAC). Use of PNF terminology and definitions is confusing in the literature,
and a full understanding of PNF theory is yet to be developed. However, it is currently believed that suppression
of the stretch reflex and enhancement of the Golgi
tendon reflex work to make this method effective. Thus, the PNF technique is
designed to capitalize on the neurological mechanisms in the muscle and joint.
There are 3 typical methods used today for
flexibility training: static, dynamic (ballistic), and proprioceptive
neuromuscular facilitation (PNF) stretching. Because temperature affects the
extensibility of the soft tissues around the joint, completing 5 minutes of
warm-up (light aerobic exercise) is recommended before performing flexibility
exercises. Static and dynamic stretching are both effective means of increasing
flexibility, but generally static stretching is considered safer and results in
less soreness of muscles. Dynamic stretching recruits the muscle spindle to
reflexively cause contraction just after the fast stretch. This may result in
small muscle tears in the muscle due to a fast/forceful transition that may not
be timed perfectly. The slow or static stretch also recruits the muscle
spindle, but at a lower response intensity so that tearing is minimized or
eliminated. Holding a stretched position for 10-30 s is usually effective. PNF
may be the most effective method that results in the least amount of
post-stretching soreness. There are several methods of engaging in PNF. Two of
these include contract-relax (CR) and contract-relax antagonist contract
(CRAC). Use of PNF terminology and definitions is confusing in the literature,
and a full understanding of PNF theory is yet to be developed. However, it is currently believed that suppression
of the stretch reflex and enhancement of the Golgi
tendon reflex work to make this method effective. Thus, the PNF technique is
designed to capitalize on the neurological mechanisms in the muscle and joint.
Procedures
to be completed prior to the lab session:
1.
Read this lab
handout and the textbook readings listed on p. 1 of this lab.
2.
On a separate
sheet of paper, use your textbook and this lab handout to write the definitions
of the terms listed under objective #1 on the previous page.
3.
Answer the
following question:
According to your text, what are the factors that determine joint ROM?
Procedures
to be completed during the lab session:
1. Jog 10 laps around the
gym. Then, work in groups of 3 to measure the ROM for the hip flexion and hip
extension as described below. Measurements should be made for each person in
the group. You should measure only the right side of the body for the purposes
of this lab. [NOTE: Bilateral measurements should be taken in an actual measurement
situation, since ROM is specific to the joint being measured.] Each measurement
should be made 3 times, and the average of the two closest measures should be calculated.You should record your measurements in
the space provided in your lab, and then transfer your average ROM to Table 1
of your lab.
Follow the specific instructions provided on the
following pages. At the endpoint of the joint ROM being measured, the axis of
the goniometer should be place on the joint axis. The
stationary arm of the goniometer should be aligned
with the proximal point of the proximal segment, and the movable arm of the goniometer should be aligned with the distal point of the
distal segment. The start position is anatomical position, which is always 0°
unless otherwise indicated, therefore, you should use
the scale on the goniometer that reads 0° in the
start position. Use the specific landmarks as indicated for each measurement.
Active ROM should created by the subject with his/her own muscle contraction.
For passive ROM, one group member should apply an external force to the distal
segment of the subject while the other group member measures ROM. When applying
this external force, be very careful not to cause any injury to the subject.
Apply the force slowly – the subject should tell you when to stop. You should
then hold the position until the measurement has been made.
Determine the ROM for flexion and hyperextension by calculating
the absolute value of the difference between your base starting position (usually
0°)
and your end position (measurement). If the subject cannot position the joint
at 0°
initially, then the ROM should be calculated as the absolute value of the
difference between the base starting position and the end position, and a note
should be made regarding the difficulty the subject had in adopting the start
position.
Hip flexion
Starting position: Subject
lies supine upon a firm, flat surface with the opposite hip held in anatomical
position. Knee should flexed maximally while
performing the movement. Do not allow
the pelvis to lift during the movement.
Goniometer placement:
Proximal point of proximal segment – lateral pelvis
midline (pointing toward GH joint)
Approximate joint axis – greater trochanter
of femur
Distal point of distal segment – lateral condyle of femur
Measurements to perform (record in Table 1):
|
|
Trial
1 |
Trial 2 |
Trial
3 |
Average
of 2 Closest |
|
Active flexion |
|
|
|
|
|
Passive flexion |
|
|
|
|
Active hip flexion
Passive hip flexion
Hip extension
Starting position: Subject
lies prone in anatomical position on a firm, flat surface. Subject should maintain contact of both iliac crests with the surface
during measurement.
Goniometer placement:
Proximal point of proximal segment – lateral pelvis
midline (pointing toward GH joint)
Approximate joint axis – greater trochanter
of femur
Distal point of distal segment – lateral condyle of femur
Measurements to perform (record in Table 1):
Active hip hyperextension
|
|
Trial
1 |
Trial 2 |
Trial
3 |
Average
of 2 Closest |
|
Active hyperextension |
|
|
|
|
|
Passive hyperextension |
|
|
|
|
Passive hip hyperextension
2. Calculate the average
active flexion and hyperextension ROM for your lab group and record these
values in Table 2.
3. Transfer the active hip
flexion ROM for each group member from Table 1 to Table 3 in the column labeled
“Position 1”. Then, measure active hip flexion for each group member using
three additional measurement positions described below. Record these values in
Table 3.
4.
In
Table 4, record the pretest hip flexion ROM from Table 3, Position 1 for each
subject. Then, perform a static stretch, a dynamic stretch, and a PNF stretch
for the hip extensors as described below. After each stretch, immediately measure
hip flexion ROM using Position 1 as described and record
it in Table 4. Each group member should perform each stretch and have ROM
measured. To reduce the order effect, the stretches should be performed in a
different order by each subject, and subjects should be allowed to rest between
each stretch. Use the following order for your group to randomize the order and
allow adequate rest between stretches:
Subject 1 – static stretch
Subject 2 – dynamic stretch
Subject 3 – PNF stretch
Subject 1 – PNF stretch
Subject 2 – static stretch
Subject 3 – dynamic stretch
Subject 1 – dynamic stretch
Subject 2 – PNF stretch
Subject 3 – active stretch
 Static stretch – Subject should
perform the modified hurdler stretch shown below to the right. Subject should sit
on the floor with the right leg straight and the left leg tucked close to the
body. Subject should reach toward the right foot as far as possible, keeping the
back straight and the right foot pointed toward the ceiling. When the subject has
reached as far as possible, have him/her hold the position for 30 s.
Static stretch – Subject should
perform the modified hurdler stretch shown below to the right. Subject should sit
on the floor with the right leg straight and the left leg tucked close to the
body. Subject should reach toward the right foot as far as possible, keeping the
back straight and the right foot pointed toward the ceiling. When the subject has
reached as far as possible, have him/her hold the position for 30 s.
Dynamic stretch – Subject should adopt
the same position as described for the static stretch. The subject should then
“bounce” back and forth, alternately reaching for the right foot (flexing the
hip) and then returning to the start position (extending the hip) in a rhthymical manner. Subject
should start with a small amount of movement and gradually increase to almost
full ROM. Continue this “bouncing” for 30 s.
PNF stretch (CRAC
method)
– Subject should lay on his/her back on the floor and bend both hips and knees
to approximately 90°. Then, subject should slowly straighten
the right knee. With the knee straight, the partner should push on the right
leg and apply a passive stretch to the hamstrings (in other words, attempt to
flex the hip of the subject). When the subject reaches the end of this passive
ROM, s/he should hold the position for 6 s. At the end of the 6 s, the subject should
contract the hamstrings against the partner’s resistance for another 6 s. At
the end of the contraction, the partner should passively push the leg into
increased hip flexion while the subject contracts his/her hip flexors to assist
the partner. When the subject has flexed the hip as far as possible, have
him/her completely relax the leg while the partner holds the subject in the new
position for 6 s.
5.
Complete
the questions at the end of the lab.
Lab Data
Sheet
Table
1. ROM for selected joints.
|
Joint |
Active
Flexion (°) |
Passive
Flexion (°) |
Active
Hyperextension (°) |
Passive
Hyperextension (°) |
|
Shoulder |
|
|
|
|
|
Elbow |
|
|
|
|
|
Hip |
|
|
|
|
|
Knee |
|
|
|
|
|
Ankle |
|
|
|
|
Table
2. Average active ROM for selected joints.
|
Joint |
Average
Active Flexion (°) |
Measured
Active Flexion (°) |
Average
Active Hyperextension (°) |
Measured
Active Hyperextension (°) |
|
Shoulder |
180 |
|
60 |
|
|
Elbow |
150 |
|
0 |
|
|
Hip |
120 |
|
30 |
|
|
Knee |
135 |
|
10 |
|
|
Ankle |
20
(DF) |
|
50
(PF) |
|
Table 3. Active
hip flexion ROM for three different positions.
|
Joint |
Position
1 (°) |
Position
2 (°) |
Position
3 (°) |
Position
4 (°) |
|
Subject 1 |
|
|
|
|
|
Subject 2 |
|
|
|
|
|
Subject 3 |
|
|
|
|
|
Average |
|
|
|
|
Table 4. Active
hip flexion ROM after three different stretching routines.
|
Joint |
Pretest
ROM (°) |
ROM
after Static Stretch (°) |
ROM
after Passive Stretch (°) |
ROM
after PNF Stretch (°) |
|
Subject 1 |
|
|
|
|
|
Subject 2 |
|
|
|
|
|
Subject 3 |
|
|
|
|
|
Average |
|
|
|
|
Questions
1.
Based
on your experiences in this lab, discuss the difficulties of using a goniometer to measure ROM and the practical limitations of
this measurement technique. Identify the most appropriate settings in which to
use goniometry.
2.
Passive
ROM is usually greater than active ROM, and active ROM usually decreases sooner
than passive
3.
We
often use the term "double-jointed" to describe a person who can move
their body parts in ways not normally possible.
What is the cause of this "phenomenon"?
4.
Use
Table 2 to compare your ROM values with the average values that are
presented. Are there any differences
between your values and the average values?
Why might those differences exist? [Hint: Consider the factors that
affect ROM described in your
5.
Select
one joint from those measured. Calculate
the total active ROM for that joint (maximum active flexion to maximum active
hyperextension) and describe two movements which normally require the entire
range of motion for both flexion and extension.
6.
Examine
the data from Table 3. Was hip flexion ROM the same or different for the 4
positions measured? Explain the similarities and/or differences you observed.
7.
According
to your data in Table 4, which stretching method is most effective at
increasing ROM? Are your findings in agreement with your text? Why or why not?
References
Adrian, M.J. & Cooper,
J.M. (1995). Biomechanics of human movement (2nd ed.).
Bridges,
J.M., & Jensen, R. (1999) Kinesiology laboratory manual. Stipes Publishing. pp.
45-56.
Eston, R., and Reilly, T.
(2001) Kinathropometry and exercise
physiology laboratory manual: Tests, procedures, and data (2nd ed). Volume 1: Anthropometry.
Hamilton,
N., & Luttgens, K. (2001). Kinesiology: Scientific
basis of human motion (10th ed.).
Kreighbaum, E., & Barthels, K. M. (1996). Biomechanics: A
qualitative approach for studying human movement (4th ed.).